Steven Struhl, MD
New York University Hospital for Joint Diseases
New York, NY
Read Dr. Struhl’s published article on Double Endobutton Technique for Repair of Complete Acromioclavicular Joint Dislocations
ABSTRACT
A gold standard for the reconstruction of the coracoclavicular complex has yet to emerge for the treatment of separation of the acromioclavicular joint. Most of the current techniques not only fail to recreate the original anatomy, but also do not use materials that are strong enough to maintain the reduction during the healing process. Using a weak and non anatomical construct has predictably led to problems with slippage of the initial reduction, as well as implant-related complications. This report introduces a novel technique for the reconstruction of complete acromioclavicular joint separation by using an Endobutton CL that has been modified for use in the shoulder. The device is placed through holes in the coracoid and clavicle reproducing the course of the conoid portion of the coracoclavicular ligament. The Endobutton CL material has been shown to have both strength and stiffness in excess of the native anatomy, ensuring a stable reduction. The procedure is simple, has low morbidity, and can be easily adapted to an arthroscopic technique.
Keywords: acromioclavicular joint, coracoclavicular ligament, AC dislocation, shoulder, AC joint
Traumatic separation of the acromioclavicular (AC) joint is common, particularly in the athletic population. Complete rupture of the coracoclavicular ligament is common to all of the more severe grades of injury (types 3 or greater). Although surgical techniques for repairing or reconstructing this ligament have evolved over the last several decades, a gold standard has not yet emerged. The weight of the arm places constant deforming force on the fixation construct during biologic healing. In the acute setting, there is a robust healing response after ligament rupture, and additional grafting may not be necessary as long as the initial fixation can remain stable during the healing process. In the chronic setting, it is necessary to add biologic graft material to the fixation construct to ensure long-term stability and function. During the healing process, graft material is likely to weaken and stretch during the course of revascularization.
Thus, when a fixation device is used in conjunction with a graft, it is at risk for implant failure if the graft deforms and stretches. The ideal procedure would use a fixation construct that not only restores the normal biomechanics of the ligament complex, but also can maintain reduction throughout the biologic healing process. This article presents a novel technique for repairing or reconstructing the coracoclavicular ligament using a device, the Endobutton CL, which has a long successful track record in anterior cruciate ligament reconstructions. The device is modified for use in the shoulder by adding a second Endobutton to the construct, creating a knotless fixation. The Endobutton is placed through holes in the clavicle and coracoid, reproducing the normal course of the conoid portion of the coracoclavicular ligament. The device may be used alone or in conjunction with a variety of biologic materials depending on whether the surgery is being performed in the acute or chronic setting. Although the current article presents an open technique, it can be modified for an arthroscopic approach using techniques that have been previously described.
SURGICAL TECHNIQUE
A 2-in incision is made from the palpable base of the coracoid tip to the anterior edge of the distal clavicle. Medial and lateral skin flaps are developed. The deltoid is split in line with its fibers, and the coracoid is identified and cleared off all the way to the base. The medial and lateral edges of the coracoid at the base are clearly identified. The clavicle is manually reduced, and while the reduction is being held, a drill tip guide wire is drilled into the top of the clavicle approximately 3 cm medial to the AC joint and midway between the anterior and posterior border of the clavicle.
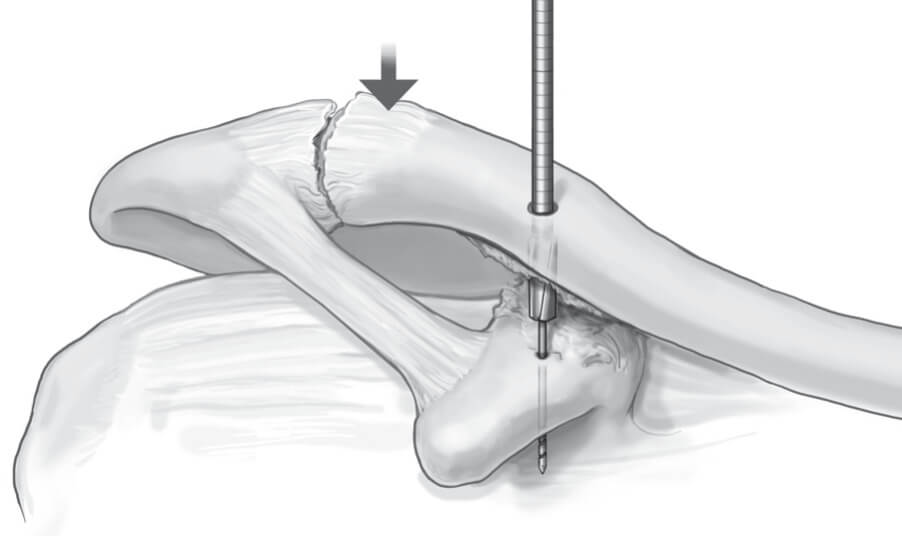
The drill hole should be directly over the base of the coracoid, and the drill should be aimed slightly anteriorly. After drilling through the clavicle, the guide wire should be easily visualized in between the clavicle and coracoid. Once the tip of the guide wire is confirmed to be entering the coracoid well centered between the medial and lateral edges, it is then drilled all the way throughout the base. The 4.5-mm Endobutton drill is now used to ream over the drill tip guide wire (Fig. 1).
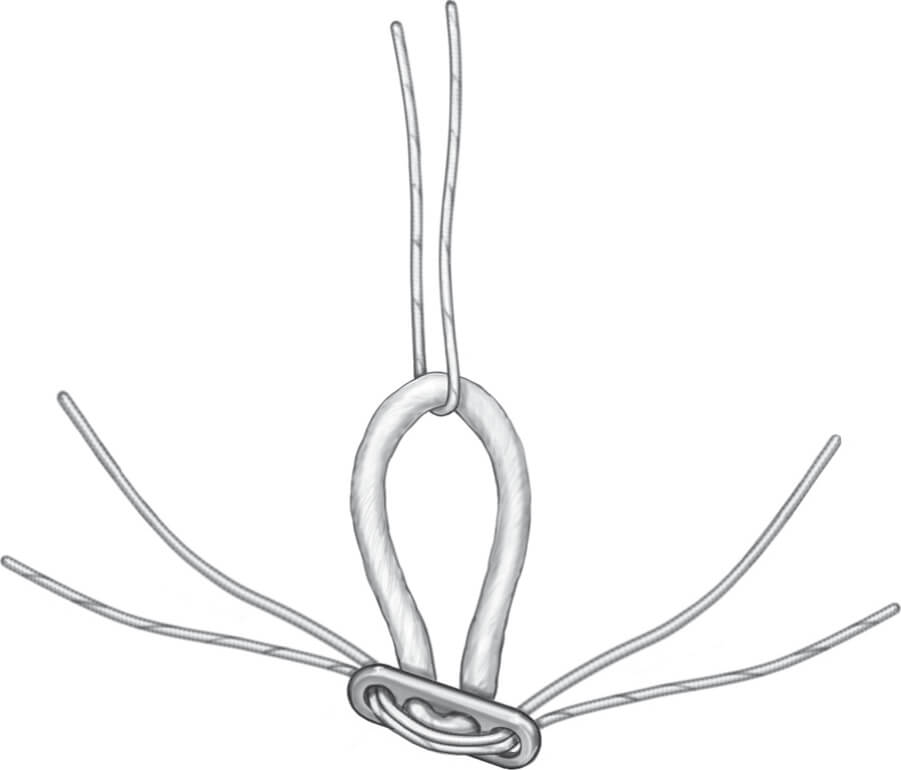
With the clavicle well reduced, the Endobutton depth gauge is used to determine the channel length. A second 2.5-mm drill hole is placed 1 cm lateral to the Endobutton drill hole. The appropriate size Endobutton CL is chosen and 2 no. 5 Ethibond (or similar) sutures are placed through the first and fourth holes of the Endobutton. A third suture is placed at the apex of the loop of the Endobutton CL. This suture is well marked so it can be identified as the loop stitch (Fig. 2).
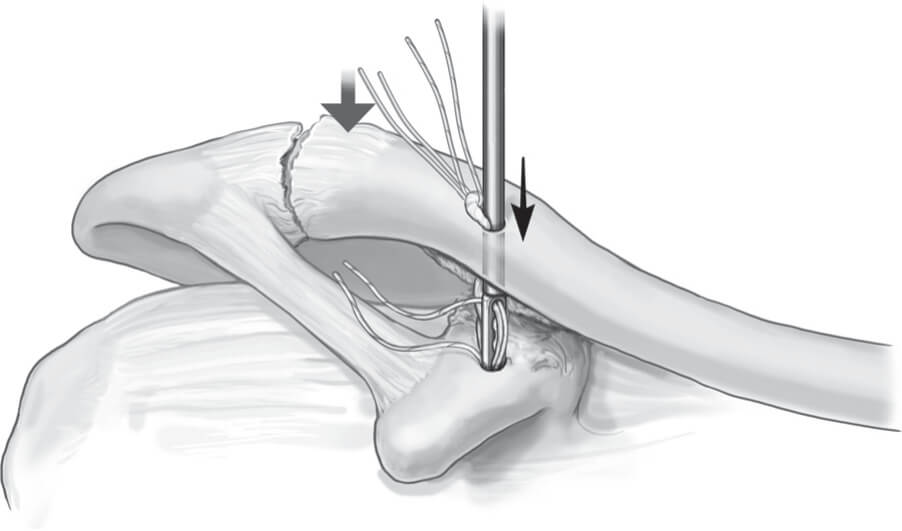
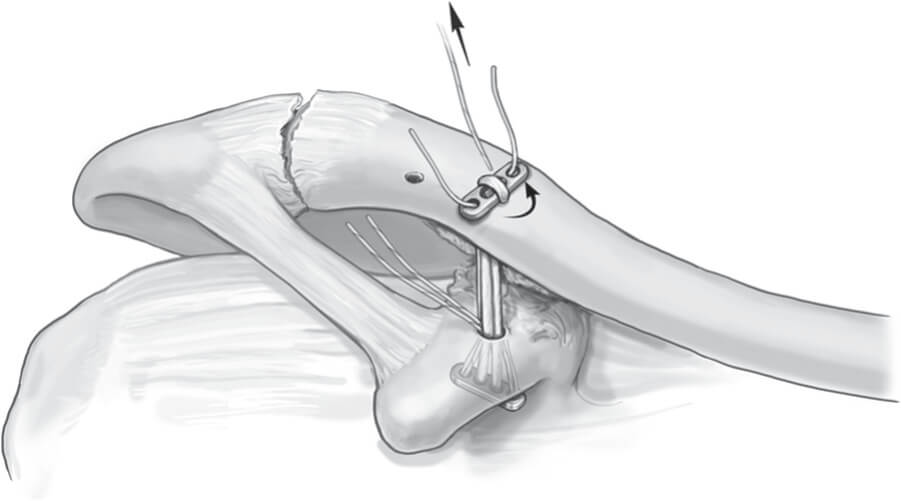
Using a 3.2-mm smooth cylindrical plunger, the Endobutton, along with its associated sutures, is pushed into the top of the clavicle through the previously drilled hole. The Endobutton is visualized in the space between clavicle and coracoid (Fig. 3) and then pushed further going into the coracoid drill hole until it ”pops” out the underside of the coracoid. The loop stitch is pulled up, locking the Endobutton onto the underside of the coracoid. One of the 2 pairs of suture tails is pulled out of the interval between the coracoid and clavicle.
This will leave 1 suture (2 tails) going from the coracoid Endobutton exiting the top of the clavicle. With firm downward pressure on the clavicle to maintain maximum reduction, the loop stitch is pulled up. With very firm upward pull on the loop stitch, the very tip of the Endobutton CL loop will be seen to be protruding from the top of the clavicular hole. A free Endobutton is held with a suture holder and is now slid into the protruding loop so that it sits centered under the loop. It is extremely important that the Endobutton be held on its edge, not lying flat against the bone. Pass the suture tails exiting the top of the clavicle through Endobutton holes (it is best to use holes 2 and 3) on either side of the Endobutton CL loop (Fig. 4).

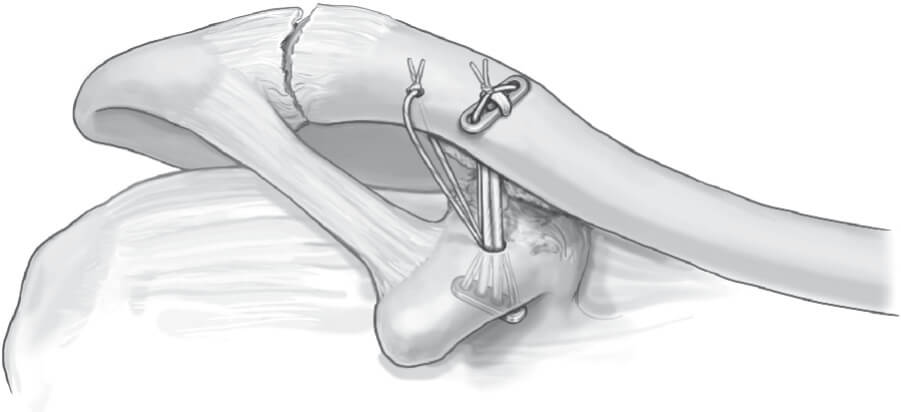
With the suture holder, now turn the Endobutton so it lays flat on the bone (Fig. 5). Tie the sutures on top of the Endobutton CL loop. This now locks the loop in place and completes the reconstruction of the conoid portion of the coracoclavicular ligament. Retrieve the suture tails that were brought out of the coracoclavicular space and pass 1 tail through the second (2.5-mm) drill hole. Tie the suture. This recreates the trapezoid portion of the coracoclavicular ligament (Fig. 6).
DISCUSSION
The initial treatment of an acute type 3 separation of the AC joint remains controversial. Although many studies have demonstrated successful outcome with nonoperative treatment, several studies have noted poor outcomes in over 40% of patients. Many of these patients have subsequent surgical treatment of ongoing symptoms of both pain and/or weakness.1-3 Long-term follow-up has shown residual symptoms in most patients treated nonoperatively.4 This has led to a commonly accepted recommendation of surgical treatment in high-level athletes or high-demand manual laborers.
However, even in patients with lower demand levels, a recent study has shown a poor outcome in 20% of non athletes, and an additional 15% of patients reported significant symptoms of weakness.5 Surgical treatment has shown much higher success rates in recent studies,6-8 however, many of the techniques have been associated with significant implant related complications.9-12 The failure to establish a gold standard with a reproducible outcome and a consistently low complication rate has led most sports medicine specialists to continue to recommend nonoperative management for the initial treatment of a type 3 AC joint separation. A recent survey of over 500 members of the American Orthopaedic Society for Sports Medicine indicated that more than 80% of respondents prefer nonoperative treatment as an initial management.13 Techniques using various forms of hardware fixation, such as the Bosworth screw, have fallen out of favor because of problems with hardware failure and the need for a second procedure to remove the hardware.
The Weaver-Dunn procedure, first described in 1972, avoids the use of metallic implants and continues to be a popular procedure. The original article however showed a failure rate of 28% in a small series of 15 patients.14 Attempts to improve the original Weaver-Dunn technique have involved various methods of nonmetallic fixation to stabilize the AC joint.15-17 Although many of these modifications have shown excellent success, implant-related problems including infection, soft tissue reactivity, and fractures have been identified.18-20 These implant-related problems have led to the development of purely biologic constructs with the use of allograft or autograft to reconstruct the coracoclavicular complex.21
Biomechanical studies have led to the development of new techniques with the goal of more accurately recreating the native anatomy and finding materials that can tolerate the cyclic loading without deformation or failure. The ultimate strength, stiffness, and load elongation curves of the native complex have been measured against various repair constructs.22-26 Testing has been done with both simple load to failure modes as well as response to cyclical loading to simulate postoperative conditions.
Traditional procedures such as the Weaver-Dunn have been shown to be much weaker and much more compliant than the native ligament leading, thereby explaining the frequently observed high failure rate of this procedure.27 Numerous modifications of the original Weaver-Dunn procedure have been evaluated with biomechanical studies. The most common modification involves stabilizing the joint by placing a cerclage material around the base of the coracoid and through a hole in the clavicle. Thick, robust materials such as polydioxanone bands or large tendon grafts have indeed shown comparable strength relative to the native complex, however, their load-elongation curves indicate lower stiffness in most of the tested materials.21,23,28,29 More importantly, cerclage techniques have also been shown to be nonanatomical as the fixation method drags the distal clavicle anteriorly. A study by Baker et al30 shows that even when the drill hole is placed within 2mm of the anterior edge of the clavicle, the clavicle is pulled anteriorly. This malreduction may likely lead to abnormal forces placed on the construct, weakening it with time as the constant cyclical forces act on it during the healing process.
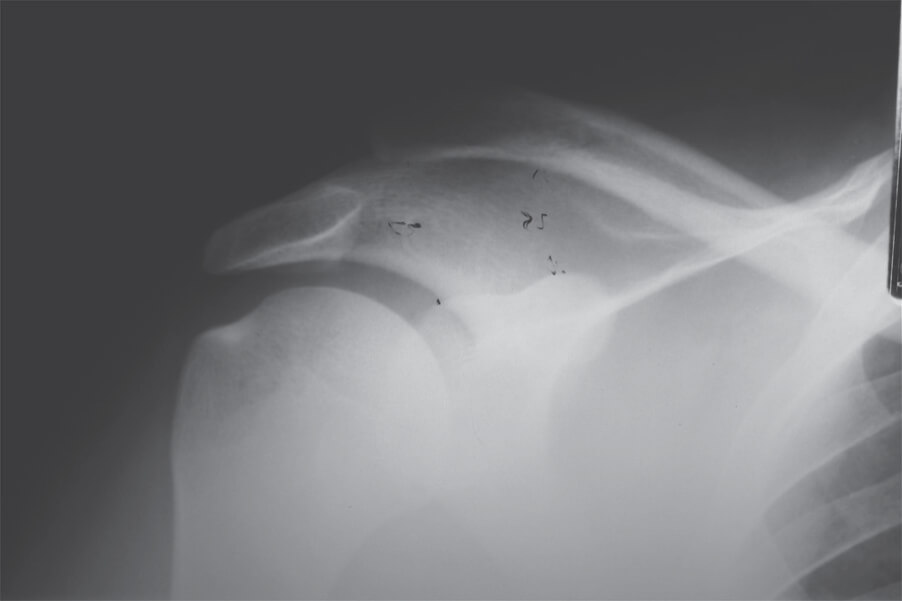
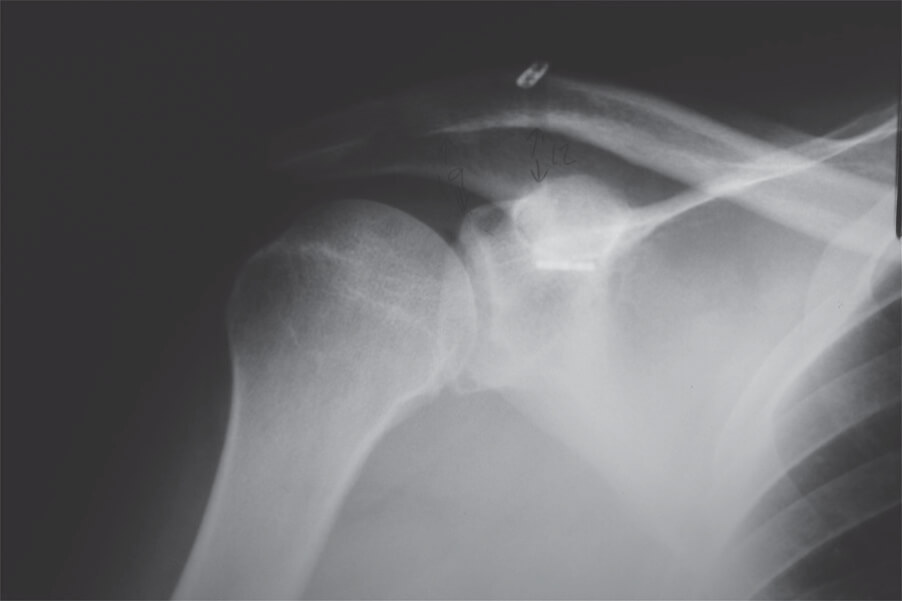
Fixation placed in anatomically correct positions may improve implant stability and response to cyclical loads. Indeed, several newer techniques have been described that achieve stability by placing grafts or fixation devices through anatomically placed holes in the clavicle and coracoid.28-31 The technique described here has been successfully used in cases of chronic type 3 or 4 AC separations (Figs. 7, 8). The Endobutton CL device is placed in an anatomically correct fashion to reproduce the course of the conoid portion of the coracoclavicular ligament.
The documented strength and stiffness of the device exceed the native ligament complex by approximately 40% (internal testing by Smith and Nephew). The deforming forces of the weight of the arm are distributed along the surface of the 2 metal Endobutton plates and not the suture material itself, which passes through the holes of the Endobutton, thereby minimizing the chance of soft tissue reaction to the suture material. Extra suture material that passes through the Endobutton holes can be used to recreate the course of the trapezoid component of the coracoclavicular ligament, thereby adding stability in the anteroposterior plane. In addition, the required drill holes are relatively small (4 mm), allowing the implant to be used either as a stand-alone device or in conjunction with other biologic implants to improve long-term stability. The suture material is a continuous loop, thereby eliminating problems of knot slippage associated with other types of suture fixation. The technique is technically straightforward and uses a small incision with minimal soft tissue dissection. Whereas this report demonstrates the validity of the procedure with an open technique, morbidity can be further reduced by adapting it to an arthroscopic approach by using previously described arthroscopic approaches to the coracoid.32, 33 Further biomechanical testing as well as clinical experience will better define the indications of this technique in the treatment of both acute and chronic AC joint separations.
REFERENCES
- Dawe CJ. Acromioclavicular joint injuries. J Bone Joint Surg Br. 1980;62:269.
- Woytys EM, Nelson G. Conservative treatment of grade III acromioclavicular dislocation. Clin Orthop Relat Res. 1991; 268:112Y119.
- Imatani RF, Hanlon JJ, Cady GW. Acute, complete acromioclavicular separation. J Bone Joint Surg Am. 1975; 57:328Y332.
- Dias JJ, Steingold RF, Richardson RA, et al. The conservative treatment of acromioclavicular dislocation: review after five years. J Bone Joint Surg Br. 1987;69: 719Y722.
- Schlegel TF, Burks RT, Marcus RL, et al. A prospective evaluation of untreated acute grade III acromioclavicular separations. Am J Sports Med. 2001;29:699Y703.
- Chernchujit B, Tischer T, Imhoff AB. Arthroscopic reconstruction of the acromioclavicular joint disruption: surgical technique and preliminary results. Arch Orthop Trauma Surg. 2006;126:575Y581.
- Dimakopoulos P, Panagopoulos A, Syggelos SA, et al. Double-loop suture repair for acute acromioclavicular joint disruption. Am J Sports Med. 2006;34:1112Y1119.
- Tienen TG, Oyen JF, Eggen PJ. A modified technique of reconstruction for complete acromioclavicular dislocation: a prospective study. Am J Sports Med. 2003;31:655Y659.
- Larsen E, Bjerg-Nielsen A, Christensen P. Conservative or surgical treatment of acromioclavicular dislocation: a prospective controlled randomized study. J Bone Joint Surg Am. 1986;68:552Y555.
- Taft TN, Wilson FC, Oglesby W. Dislocation of the acromioclavicular joint: an end-result study. J Bone Joint Surg Am. 1987;69:1045Y1051.
- Tsou PM. Percutaneous cannulated screw coracoclavicular fixation for acute acromioclavicular dislocations. Clin Orthop Relat Res. 1989;243:112Y121.
- Calvo E Lopez-Franco M, Arribas IM. Clinical and radiologic outcomes of surgical and conservative treatment of type III acromioclavicular joint injury. J Shoulder Elbow Surg. 2006;15:300Y305.
- Nissen CW, Chatterjee A. Type III acromioclavicular separation: results of a recent survey on its management. Am J Orthop. 2007;36:89Y93.
- Weaver JK, Dunn HK. Treatment of acromioclavicular injuries, especially complete acromioclavicular separation. J Bone Joint Surg Am. 1972;54:1187Y1194.
- Morrison DS, Lemos MJ. Acromioclavicular separation: reconstruction using synthetic loop augmentation. Am J Sports Med. 1995;23:105Y110.
- Hessmann M, Gotzen L, Gehling H. Acromioclavicular reconstruction augmented with polydioxanonsulphate bands: surgical technique and results. Am J Sports Med. 1995;23:552Y556.
- Weinstein DM, McCann PD, McIllveen SJ, et al. Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med. 1995;23:324Y331.
- Stewart AM, Ahmad CS. Failure of acromioclavicular reconstruction using Gore-Tex graft due to aseptic foreignbody reaction and clavicle osteolysis: a case report. J Shoulder Elbow Surg. 2004;13:558Y561.
- Boldin C, Frankhauser F, Ratschek M, et al. Foreign-body reaction after reconstruction of complete acromioclavicular dislocation using PDS augmentation. J Shoulder Elbow Surg. 2004;13:99Y100.
- Guttman D, Paksima NE, Zuckerman JD. Complications of treatment of complete acromioclavicular joint dislocations. In: Price CT, ed. Instructional Course Lectures 49. Rosemont, IL: American Academy of Orthopedic Surgeons; 2000: 407Y413.
- Lee SJ, Nicholas SJ, Akizuki KH, et al. Reconstruction of coracoclavicular ligaments with tendon grafts: a comparative biomechanical study. Am J Sports Med. 2003;31:648Y654.
- Jerosch J, Filler T, Peuker E, et al. Which stabilization technique corrects anatomy best in patients with ACseparation: an experimental study. Knee Surg Sports Traumatol Arthrosc. 1999;7:365Y372.
- Motamedi AR, Blevins FT, Willis MC, et al. Biomechanics of the coracoclavicular ligament complex and augmentations used in its repair and reconstruction. Am J Sports Med. 2000;28:390Y394.
- Harris RI, Wallace AL, Harper GD, et al. Structural properties of the intact and the reconstructed coracoclavicular ligament complex. Am J Sports Med. 2000;28: 103Y108.
- Wickham MQ, Wyland DJ, Glisson RR, et al. A biomechanical comparison of suture constructs used for coracoclavicular fixation. J South Orthop Assoc. 2003;12:143Y148.
- Deshmuckh AV, Wilson DR, Zilberfarb JL, et al. Stability of acromioclavicular joint reconstruction: biomechanical testing of various surgical techniques in a cadaveric model. Am J Sports Med. 2004;32:1492Y1498.
- MacDonlad P, Sunner P, Dyck M. A follow-up of surgical treatment of type III AC dislocations. Paper presented at: the closed ASES meeting 2006.
- Grutter PW, Petersen SA. Anatomical acromioclavicular ligament reconstruction: a biomechanical comparison of reconstructive techniques of the acromioclavicular joint. Am J Sports Med. 2005;33:1723Y1728.
- Costic RS, Labriola JE, Rodosky MW, et al. Biomechanical rationale for development of anatomical reconstructions of coracoclavicular ligaments after complete acromioclavicular joint dislocations. Am J Sports Med. 2004;32:1929Y1936.
- Baker JE, Nicandri GT, Young DC, et al. A cadaveric study examining acromioclavicular joint congruity after different methods of coracoclavicular loop repair. J Shoulder Elbow Surg. 2003;12:595Y598.
- Mazzocca AD, Santangelo SA, Johnson ST, et al. A biomechanical evaluation of an anatomical coracoclavicular ligament reconstruction. Am J Sports Med. 2006;34: 236Y246.
- Wolf EM, Pennington WT. Arthroscopic reconstruction for acromioclavicular joint dislocation. Arthroscopy. 2001;17: 558Y563.
- Baumgarten KM, Altchek DW, Cordasco FA. Arthroscopically assisted acromioclavicular joint reconstruction. Arthroscopy. 2006;22:228.e1Y228.e6.